
Our thoughts on ear infections, antibiotics and ear fluid
by Matt Lando MD, with Foreward by Ann Smith, MD
Foreward
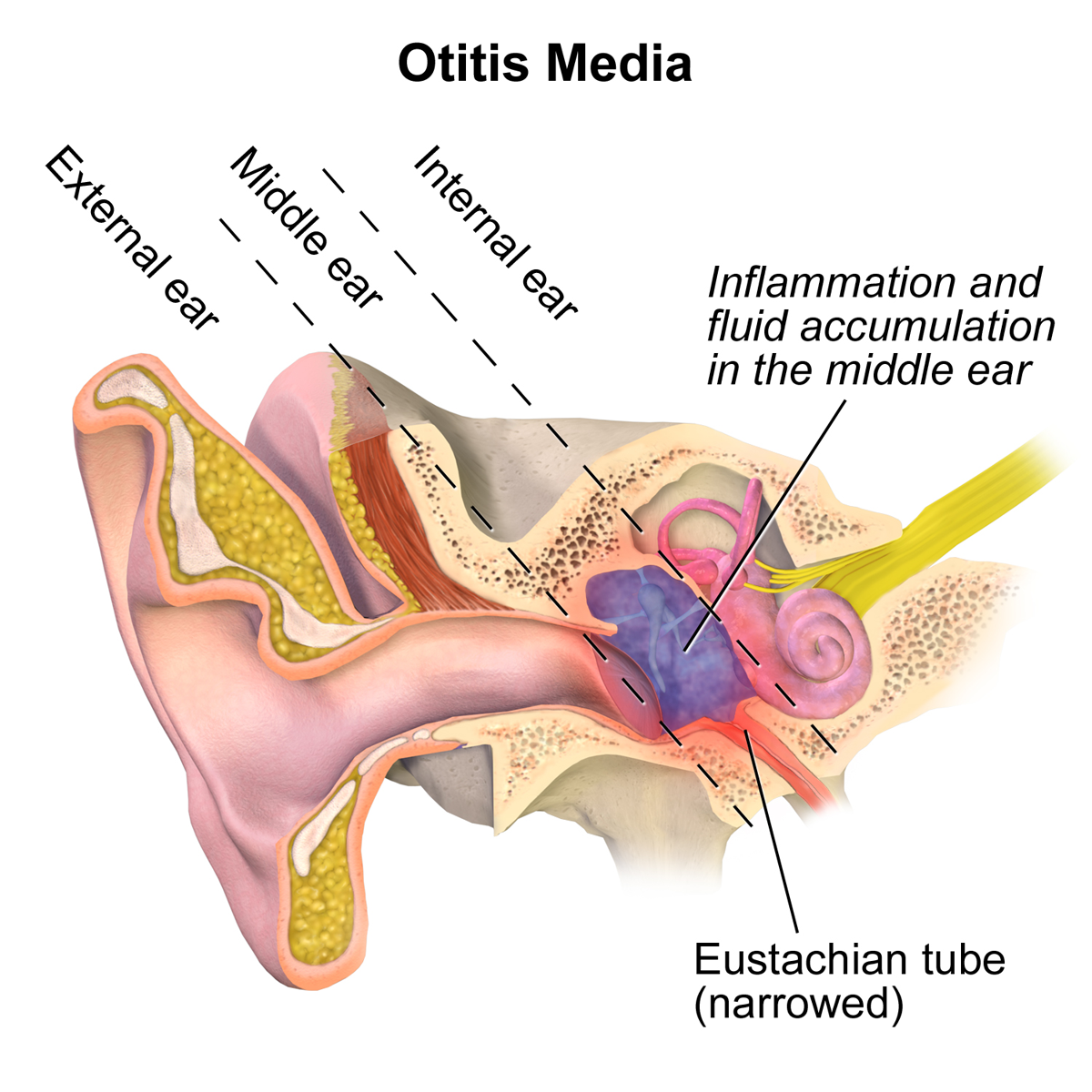
First, some definitions and clarification. The middle ear is the air-filled space behind the eardrum with the vibrating ossicles (ear bones) that amplify and transmit soundwaves into the inner ear hearing organ. Otitis media as a general term refers to disease in the middle ear space. It includes both acute otitis media (AOM) and otitis media with effusion (OME).
Acute otitis media is an infection, either bacterial or viral. It causes swelling of the lining tissue and infected mucus to fill the middle ear space, blocking sound. Treatment with antibiotics can shorten the symptoms of bacterial infection, but many cases improve without antibiotics. There is no role for antibiotics in viral infections ( common colds ). Otitis media with effusion is fluid that is not infected, but also blocks sound. There are often only mild symptoms of pressure sensation or other ear discomfort. Otitis media with effusion occurs in several ways. It is the natural after effect of ear infection, and the reason why hearing is still poor even when pain, fever and inflammation have resolved. In most cases, this fluid will gradually be absorbed or cleared and replaced by air over several weeks. No medications have been shown to be helpful in speeding up this process. If the fluid does not clear after 3 months and hearing is still blocked, treatment is recommended. Allergies can also cause OME from inflammation and increased fluid production. Eustachian tube dysfunction can cause fluid on its own, and is an underlying cause for persistent fluid after infections or allergy attacks. The normal function of the Eustachian tube is to regulate the amount of air that is in the middle ear space. Equal pressure on either side of the eardrum allows it to vibrate freely and transmit sound. The Eustachian tube is normally collapsed and only opens through action of muscles in the palate. Eustachian tubes don’t work well in children due to shape of their heads and immaturity of the immune system. This is why fluid can last for a long time and takes longer to clear than in adults. Unfortunately, the resulting hearing loss affects speech and language development in particular and learning in general. What follows below is a summary of the medical literature and current treatment of otitis media
###################
Acute otitis media remains one of the most common diseases of infancy and early childhood on a world wide basis and is a leading cause of health care visits and drug prescriptions. Otitis media with effusion (OME) is the leading cause of hearing impairment in children in developed nations (1).The burden of disease worldwide in 2012 was estimated to be 709 million cases each year with 51% of these cases occurring in patients <5 y/o (2). 75% of children experience at least one ear infection before starting school (3). Otitis media is a common reason for visits to pediatricians offices accounting for >11% of office encounters in primary care practices(4). Otitis media is the most common condition for which antibiotics are prescribed to children in the United States with the rate being almost 80% of OM visits resulting in antibiotic prescriptions (5). According to the clinical practice guidelines for OME, "direct costs related to otitis media, which includes OME and AOM, are $3 billion to $5 billion annually, and the true economic impact is likely to be higher, because indirect costs are sizable and yet difficult to estimate "(6). Because of the prevalence of OM and the significant medical sequelae and associated high financial costs, many countries now have guidelines for the clinical management of OM. "In almost all, the public health goal of containing acquired resistance in bacteria through reduced antibiotic prescribing is the main aim and basis for recommendation" (7). Despite the time, effort, and expense in developing these guidelines and educating the clinicians, the guidelines are not followed closely and their aim is not achieved (7). In the US, "only 7% to 33% of pediatricians use pneumatic otoscopy for diagnosis, and only 29% obtain an age-appropriate hearing test when the effusion persists for >3 months" (6). Surprisingly, 32% of pediatricians use antibiotics to treat OME, a condition for which antibiotics are strongly discouraged (8,9).
The reason for the failure of physicians to follow otitis media best practice guidelines is probably multifactorial, but one of the main contributing factors is the difficulty in making the correct diagnosis. There is a spectrum between OME and AOM that will always preclude a gold standard for diagnosing AOM. The exam can be difficult because of small canals and cerumen limiting the view of the tympanic membrane. A febrile child will have injection of the vessels of the TM which can sometimes give the impression of AOM even when there is no fluid actually present in the middle ear space.
There has been much focused work on trying to increase the sensitivity and specificity of diagnosing otitis media. One would think that ear pain, tugging at the ears, fever and irritability would be good indicators or AOM, but multiple studies have demonstrated symptoms do not correlate with an initial diagnosis of AOM(10-12). While signs such as a cloudy, bulging TM with impaired mobility have been the best predictor of AOM, there is a spectrum in all of these signs making the diagnosis difficult. The American Academy of Pediatrics has a diagnostic action statement that "AOM should not be diagnosed when pneumatic otoscopy and/or tympanometry do not show middle ear effusion", but we know that in practice these tools are not used the majority of the time due to lack of equipment and/or proficiency in the exam. When there is uncertainty in the diagnosis and the clinician is faced with an unhappy, uncomfortable child and concerned, anxious parents, clinicians generally treat with antibiotics. The most recent AOM guideline from the American Academy of Pediatrics has removed the "uncertain diagnosis" category in the belief that the presence of such a category "might condone incomplete visualization of the TM or allow inappropriate antibiotic use"(13).
There is no doubt that antibiotics are used too often for the treatment of acute otitis media in this country. Antibiotic use for AOM varies from 56% in the Netherlands to 95% in the USA, Canada, and Australia.(14) The benefits of antibiotics must be weighed against the risks as for every 14 children treated with antibiotics one child experiences an adverse event such as rash, vomiting or diarrhea that otherwise would not have occurred. The natural history of AOM is quite favorable with AOM symptoms without antibiotics improving in 61% of children within 24 hours and 80% by 2 to 3 days (15). For most children with mild disease, an expectant observational approach is advocated(14). In the case of OME, there is little indication ever for the use of antibiotics(9).
The question remains, how can the ability to correctly diagnosis and manage otitis media be improved so appropriate therapy can be instituted and inappropriate antibiotic use decreased. With time constraints increasing in medical school and residencies, it seems unlikely that proficiency in physical diagnosis, including pneumatic otoscopy, will improve. Tympanograms will continue to have the same deficiencies that occur when cerumen is present or the probe abuts the canal wall. Two areas that offer potential improvement and are currently underutilized are parent education and play audiometry. When parents bring their sick, febrile child to the clinician they want something to alleviate the problem, and can see the failure to prescribe antibiotics as a withholding of therapy. The physician-parent relationship can be further compromised because clinicians often see otalgia as a peripheral concern not requiring direct attention (16). While no one would advocate withholding antibiotics in all children with AOM and risk the suppurative complications seen in the pre antibiotics era, there is a spectrum of disease in AOM with a large percentage not requiring antibiotic therapy. "In numerous studies, only approximately one-third of children initially observed received a rescue antibiotic for persistent or worsening AOM,suggesting that antibiotics could potentially be reduced by 65% in eligible children"(13). If the child's otalgia is treated with analgesics, which does provide symptomatic relief within the first 24 hours unlike antibiotics, and the parents are educated on the potential adverse effects of antibiotics such as nausea, vomiting, rashes, deleterious effects on patient gut flora, and antibiotic resistance, there is a much greater chance they would be amenable to initial observation and less demanding of antibiotic therapy initially and especially on follow up if effusion is still present.
Play audiometry has a role as an initial diagnostic aid and as important monitor for hearing loss weeks later. Audiometry has not to this point been used on a large scale for help in diagnosing otitis media. Prior to an effective play audiometry game, the time and expense of obtaining an audiogram did not justify using audiometry as an aid in diagnosis of otitis media. An ill child presenting with a normal audiogram is certainly at a lower risk of having middle ear fluid and thus less likely to be considered for antibiotic therapy for AOM. In those children with AOM, surveillance to document resolution of fluid is important, While it is not uncommon for OME to occur without hearing loss, a type B tympanogram has a sensitivity of 65% to 92% and a specificity of 43% to 80% for associated hearing loss(17), those patients without hearing loss would not be considered for therapy but periodically followed to make sure there was no structural damage to the tympanic membrane resulting from the OME. As states earlier, the majority of children with effusions persisting 3 months or longer are not tested for hearing deficits. The play audiometry would provide an easy and effective screen for monitoring the hearing in these children. The nature of the test itself would avoid the anxiety, expense, and inconvenience of going to the clinicians office, and assure the metric for assessing hearing after acute otitis media is met. Good hearing is the foundation children need to build the communication and attention skills that are needed to succeed in school and life. We are only recently becoming aware of the truly significant consequences of temporary hearing loss, including unilateral conductive hearing loss. Amblyaudia is a relatively new subcategory of auditory processing disorders. It is characterized by asymmetrical auditory processing and can result in speech and reading difficulties, information processing deficits, and inattention. Children suffering with this condition are often misdiagnosed with learning disorders and attention deficit hyperactivity disorder. Amblyaudia has been associated with conductive hearing loss and with prolonged periods of temporary hearing loss from otitis media in early life(18).
Innovative new solutions are needed to aid in the diagnosis and management of otitis media. Parent education is key to improving outcomes and maintaining the physician-parent relationship, especially with the possible perception there is withholding of care in favor of the broader public issue of reducing costs as well as containing acquired resistance in bacteria through appropriate reductions in antibiotic prescribing. Kids Hearing Game provides useful audiologic information without the costs, anxieties or inconvenience of more traditional audiometric modalities. The accessibility of this audiometric information makes it a feasible tool to aid in the diagnosis of otitis media and well as a way to meet metrics of hearing assessment and avoid delay in diagnosis of hearing loss with the subsequent development of learning disorders and school difficulties.
References
1. Qureishi A, Lee Y, Belfield K, Birchall JP, Daniel M. Update on otitis media:prevention and treatment. Infect Drug Resist. 2014;(7):15-24
2. Monasta L, Ronfani L, Marchetti F, et al. Burden of disease caused by otitis media:systematic review and global estimates. PlosONE. 2012 vol.7,issue 4
3. Vergison A, Dagan R, Arguedas A, et al. Otitis media and its consequences: Beyond the earache. Lancet infect Dis. 2010:10(3):195-203
4. Berkman ND, Wallace IF, Steiner MJ et al. Otitis media with effusion:Comparative effectiveness of treatments. Comparative effectiveness review No. 101, Rockville, MD:Agency for Healthcare Research and Quality;2013
5. Grijalva CG, Nuorti JP, Griffin MR. Antibiotic prescription rates for acute respiratory tract infections in US ambulatory settings. JAMA. 2009;302(7):758-766
6.Rosenfeld RM, Shin JJ, Schwartz SR, et al. Clinical practice guideline:otitis media with effusion(update). Otolaryngology-Head and Neck sure. 2016:154(1S)
7. Haggard M. Poor adherence to antibiotic prescribing guidelines in acute otitis media- obstacles, implications, and possible solutions. European Journal of Pediatrics. 2011. 170(3)323-332.
8. Lannon C, Peterson LE, Goudie A. Quality measures for the care of children with otitis media with effusion. Pediatrics. 2011; 127:e1490-e1497.
9. Venekamp RP, Burton MJ, van Dongen TM et al. Antibiotics for otitis media with effusion in children. Cochrane Database Syst Rev. 2016 Jun12;(6)
10. Shaikh N, Hobeman A, Paradise JL, et al. Development and preliminary evaluation of a parent-reported outcome instrument for clinical trials in acute otitis media. Pediatric Infect Dis J. 2009;28(1)5-8
11. Laine MK, Tahtinen PA, Ruuskanen O, et al. Symptoms or symptoms-based scores cannot predict otitis media at otitis-prone age. Pediatrics. 2010;125(5)
12. Friedman NR, McCormick DP, Pittman C, et al. Development of a practical tool for assessing the severity of acute otitis media. Pediatric Infect Dis J. 2006;25(2):101-10
13. Lieberthal AS, Carroll AE, Chonmaitree T, et al. The diagnosis and management of acute otitis media. Pediatrics. @013;131(3)
14. Venekamp RP, Sanders SL, Glasziou PP, et al. Antibiotics for acute otitis media in children. Cochrane Database Syst Rev. 2015 Jun 23;(6)
15. Rosenfeld RM, KayD. Natural history of untreated otitis media. Laryngoscope. 2003;113(10):1645-57
16. Schechter NL. Management of pain associated with acute medical illness. In: Schechter NL, Berde CB, Yaster M, meds. Pain in infants, children and adolescents. Baltimore, MD:Williams and Wilkins; 1993:537-538
17. MRC Multicenter Otitis Media Study Group. Sensitivity, specificity, an predictive value in tympanometry in predicting a hearing impairment in otitis media with effusion. Colin Otolaryngol. 1999;24:294-300
18. Whitton JP, Polley DB. Evaluating the perceptual and pathophysiological consequences of auditory deprivation in early postnatal life: A comparison of basic and clinical studies. Journal of the association for research in otolaryngology. 2011;(12)535-546